
Cheat Sheet: Build Muscle + Lose Fat in Menopause
Question: “Can I build muscle and lose fat during menopause?”
Answer: Yes, you can!
The strategy is no different in any phase of menopause
than it is for someone in their 20s, or for that of a man.
But it requires a more deliberate approach than before menopause.
Here’s How
Step 1. Manage Menopause Symptoms
Menopause - related sleep disruptions and fatigue will lead to decreased physical activity, increasing body fat.
These Help Manage Menopause Symptoms:
Menopause Hormone Therapy (MHT = Estrogen + Progesterone, Testosterone)
Or Non-hormone treatments for Vasomotor Symptoms
Strict sleep hygiene
Reduce/eliminate alcohol
Step 2. Trigger Building + Recovery
Consistently practice behaviors that trigger the body to “decide” to utilize food for building lean tissue.
Adequate & good quality Sleep
Lifting Weights — 2-4 times per week
Enough Protein — 0.7 - 0.8 grams per pound of body weight
Enough Carbs — 1 - 2.5 grams per pound of body weight
3. Keep the Sink Un-Clogged
Practice behaviors that will promote building & recovery to continue.
N.E.A.T. -- Non-Exercise Activity Thermogenesis, AKA whole body movement. 6-8K steps per day.
Hydration — Drink to thirst, or if doing endurance activities/sports meet an oz. goal
Fiber - 14 gram per 1000 Kcals, ~22 - 35g
4. Play the Long Game
6 Months in: most people start to notice the hint of change in how clothes fit.
2 Years in: others start to notice.
After two years, progress slows, but is still possible with progression, consistency, & patience.
What to do if you don’t want to see actual change

These methods = Rearranging the deck chairs on the Titanic
Try to ignore away menopause symptoms, or ‘wait them out.’
Believe in Spot reduction. Example: doing ab exercises to lose belly fat.
Try to eat less. Menopause requires better fueling, not more restriction.
Expect any benefits from Supplements like caffeine, Omega-3 s, adaptogens, vitamin infusions, probiotics, oral peptides, botanicals like Black cohosh, stimulants like L-Carnitine, Collagen protein…
Tell yourself it’s too late to start making changes. It’s never too late!
Change nothing because you can’t do every single step “perfectly.”
BREAKDOWN: Why we gain weight in mid-life
It’s more complex than calories in/out.
Reason 1. “Effects of Aging”
Weight gain is primarily driven by muscle loss, reduced physical activity, and inadequate protein intake. Which becomes a vicious cycle. PMID: 35574515 PMID: 12145025, PMID: 26883880
In the US, adults gain an average of 0.5 - 2 pounds per year through mid-life. Women typically gain weight at a higher rate and for a longer duration than men.
While men gain weight in a gradual & linear pattern, women tend to gain weight before and after the menopause transition (MT), with a redistribution of fat mass during MT. PMID: 1985614
TLDR: women & men are more likely than not to gain weight and body fat in midlife.
Women gain more weight than men, on average.
Also note: this is population research data, and may not represent you. Approx. 50-80% of Americans don’t meet recommended nutrition and physical activity guidelines.
Effects of Menopause & Hormone Therapy
Menopause doesn’t directly cause weight gain. 30843880, 22978257, 11910598, 10746891
It does increase signals for the body to lose muscle and gain fat, altering relative body composition. PMID: 30843880, 34898344, 11004935
Hormone Therapy alone doesn’t stop muscle loss, fat accumulation, or weight gain. PMID: 12055317
TLDR: Menopause is not responsible for weight gain during menopause, and has
a modest but statistically significant influence on body composition changes.
“If Menopause supposedly plays no role in weight gain,
but women gain more weight than men in the long-term, what is to blame?”
Hypothesis:
Women tend to gain more weight due to the contribution of menopause-caused body re-composition (muscle decrease & fat increase), in addition to the debilitating effect of Menopause Symptoms, and “effects of aging.”
Also, the location of fat accumulation within the few years preceding and following Menopause is insidiously unique.
During this 3-6 year time period, the body biases fat to accumulate between organs & muscle cells. Studies show it’s not much, around 3 pounds on average in the largest population study to-date. But this significant uptick in fat accumulation around Menopause has a dramatic & lasting snowball effect for long-term metabolic flexibility.
Let’s Investigate this Effect, from Inside the Body
Nutrient Partitioning = What your body is signaled to do with food every time you eat.
Your Body has Two Partition Options:
1) Partition toward storage (into subcutaneous fat or visceral/abdominal fat)
2) Partition toward functional tissue (for muscles, bone, organs)
The more consistently your body is signaled to direct nutrients toward functional tissue (muscle, bone, and energy use) rather than storage, the more likely it is to limit excess fat accumulation.
Increased visceral and intramuscular fat storage biases a “storage” signal, working in opposition to any “Functional Tissue” signals your nutrition and exercise may be sending.
This is true at any time, including menopause.
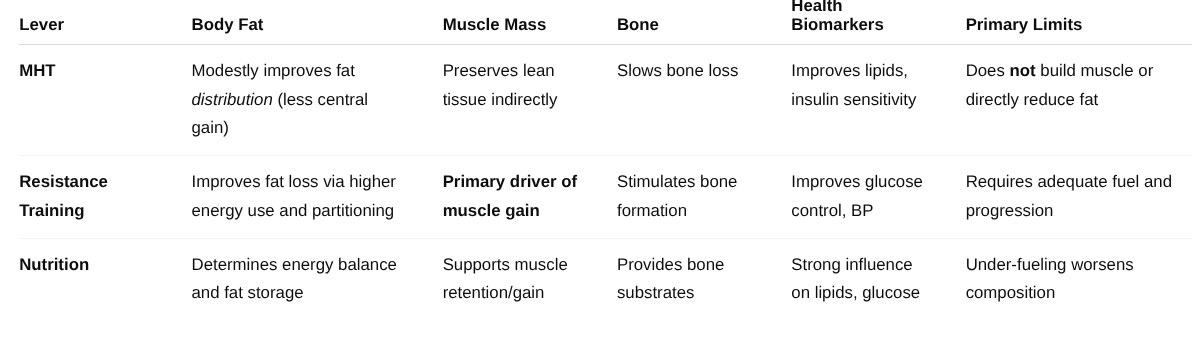
Here's a simple breakdown of the contribution from Hormone Therapy (MHT), Lifting Weights (Resistance Training), and what you eat (Nutrition).
Hormone Therapy is framed as protective, not transformative
Training is clearly the anabolic and structural driver
Nutrition is positioned as the enabler or limiter, not a stand-alone fix
🎥 Outline: Video 1.
"Menopause doesn't cause weight gain." "Hormone Therapy doesn't stop it."
- Are we sure about that? I did a lot of digging into the studies, and
- It turns out both statements are strongly supported by research.
AND we still haven't answered the question:
"Then what IS causing weight gain?"
Now. The Average American gains 1/2 - 2 pounds through mid-life.
What ELSE changes besides Menopause?
---> Let's set aside Menopause and discuss NUTRIENT PARTITIONING
NP illlustrates what your body is signaled to do with the food you eat:
1. MOBILIZE toward functional tissue like muscle, bone, & organs
2. SEND toward storage in the fat cells.
It turns out that how each body is signaled to use food is greatly effected by behavior + time.
These three factors are most responsible for an increase in NP signals for food storage:
- Decreased physical activity
- Inadequate protein intake
- Muscle loss
And it's MORE COMPLEX than a calories in/out problem, because those changes cause adaptations to our body's behavior on a physiological level.
So we don't get into the Vocabulary Weeds, let's summarize the effect of these factors as glomming up biological systems that would otherwise partition toward functional tissues.
Meaning: If you don't use it, you lose it—and if you lose it, you're less likely to use it. To boot, this 'muscle-movement loop' is accelerated or diminished by how much protein you're consistently eating.
Now insert Menopause:
Sleep Suffers, Fatigue, hot all the time >> further decreasing activity levels
No Estrogen = muscle loss + increased belly fat.
EDITING THAT PROCESS is possible
Want to learn what changes *work* and what doesn't? Click the Heart & Subscribe!
Signals for Storage
Life Events / Context
Aging with progressive lean mass loss
Menopause Transition
Unplanned & prolonged injury or illness
High-stress life phases (caregiving, job strain, burnout, emerging diagnoses)
Sleep disruptions (hot flashes, insomnia)
Behaviors
Chronic caloric restriction or dieting
Skipping meals / irregular eating
Low protein intake
Avoiding carbohydrates, particularly if training or under excess stress
Reduced overall activity level
Not resistance training
Or training inconsistently (averaging < 2 resistance training sessions per week)
What these trigger downstream:
↑ cortisol, ↓ insulin sensitivity, ↓ muscle signaling, ↓ metabolic flexibility → preferential fat storage (often central).
Signals for Helping Functional Tissue
(Muscle, bone, metabolic health)
Life Events / Context
Resistance training adoption or resumption
Recovery from under-fueling
Hormonal stabilization (including appropriate MHT use)
Improved sleep continuity
Transition out of high chronic stress
Behaviors
Resistance training that is Progressive in nature
Eating enough total energy to support training
Adequate protein intake, distributed across the day
Carbohydrate intake matched to activity demands
Consistent meal timing
Prioritizing sleep and recovery
Maintaining enough daily movement (NEAT)
Observing Rest Days
What these trigger downstream:
↑ insulin sensitivity, ↑ anabolic signaling, ↑ lean mass retention → nutrients routed toward use rather than storage.