

“Aaaugh, I’m Injured!”
A Guide to dealing with Soft Tissue Injuries
Injuries Happen
First off, nobody can “avoid injury.” It’s just not humanly possible. We can all mitigate our injury risk.
Second, whether you chose to rest it or rehab it, most injuries feel better in <16 weeks. If you choose to rest it, you’re choosing to remain highly susceptible to re-injury.
Thirdly: If you’re in Peri-Menopause+, it’s not your Imagination. When bodies stop producing estrogen, the threshold for injury and inflammation drops, and voila, it feels like — or is — one thing after another!
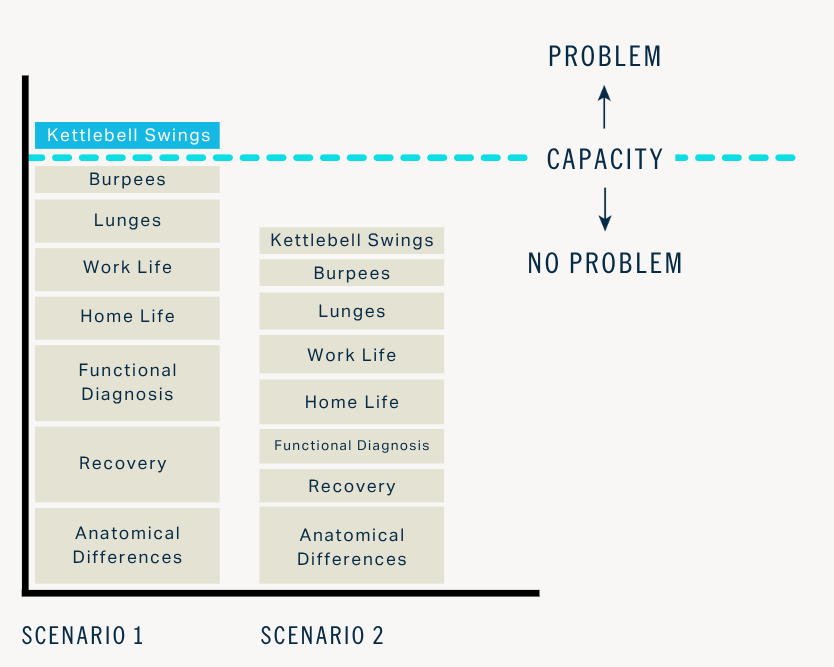
Image: “Active Life Professionals” Level 1 Seminar
How Injuries Happen
Injuries aren’t caused by “bad form.”
Injuries aren’t fault of a single exercise performed in one moment (coughs: 😮💨Deadlift).
Injuries occur when training demands exceed your current capacity.
In the example here, the cause of injury was not anything about doing the Kettlebell Swings
Rather, KB Swings were the point at which overall demand exceeded the individual’s capacity.
Gradual onset injuries (“lately I’ve been having this XYZ pain”) happen via the same mechanism as acute injuries, just at a more insidious rate.
Post-Injury: Your Comeback Starts Here

Image from The Running Clinic c/o The British Journal of Medicine
What to do: Days 0 - 3 Post-Injury
Promote blood flow & organized movement:
Daily cardio, like walking, stationary bike, etc. (while accommodating injury).
Restrict your activity only enough to mitigate re-injury or prevent additional swelling of injured fibers.
Movement: (CARs) or other movement through the injured joint’s active range of motion, up to 3×2 min. daily.
Consider increasing protein intake from 0.7 grams/pound to 15-40% higher.
If strained tissue, aim for 0.8 - 0.9 grams/pound of body weight/day
If rehab is involved: 0.9 - 1.0 grams/pound of body weight per day
If surgery recovery: 1.0 - 1.1 grams/pound of body weight per day
*Consider taking OTC Painkillers if pain is interrupting sleep, you find yourself severely restricting your movement to avoid pain/jolts.
Tylenol at the high end of the recommended dosage (but never more than 4000mg in 24 hours), for as long as you’re serving the needs listed above.
Ibuprofen at the low end of the recommended dosage, for the shortest duration necessary (to avoid GI bleeding, kidney damage, & cardiovascular issues).
What to do Days 4+ Post-Injury
1. Get back into your Training Routine
Your usual training routine should resume as soon as possible, as early as 1-3 days after an injury.
The injury will recover better — and feel better — when you stimulate your body to allocate food toward building and repairing (via training), versus ‘taking a break,’ which signals your body to send nutrients to storage in fat cells.
Training as usual for unaffected areas
Load Management / Exposure Reduction for injured tissue
Adjust exercise set-up to mitigate load on injured tissue
Adjust technique to decrease aggravating progress (i.e., shorten jogging stride length while adductor heals)
Cardio: intentional walks, bike rides, cardio machines - even ridiculously slow - will stimulate anabolic & oxidative nutrient partitioning.
2. Start Training your Injury
“The best predictor of future injury is previous injury”
Spoiler: If your entire post-injury approach is to rest the injured area and sign up for passive therapies such as massage, cupping, acupuncture, etc. you have a dang high likelihood of incurring the same injury again.
Early movement and loading accelerates recovery and improves long-term outcomes compared to rest.
Rebuilding the injured tissue should look just like any other part of your lifting routine except that you start at a different point on the continuum.
How to Re-Train Injured Soft Tissue
This part is 100% something you can do most effectively with the help of a Physical Therapist or other qualified professional. Ask me for recommendations.
Training injured soft tissue — such as a cranky tendon around the knee, pulled hamstring, or torn finger tendon — follow the same step-wise path.
Step 0. Load Management
Initially remove or modify aggravators in current training routine
1. Circulation + Active Range of Motion
No-to-low-load movement
2 minutes for 2+ times per day
Examples: Breathing drills, CARs, moving unloaded joints through active range of motion
2. Isometric Loading
Isometric = no movement
Yielding (holding a position against gravity) → overcoming (applying force against an immovable object)
Start at mid-range → progress to longer lengths/end-ranges
Example Squat hold halfway down
3. Controlled Isotonics
Isotonic = Moving through gradually increasing ranges of motion
Slow controlled tempo
Example: Tempo Goblet squats to a bench
4. Lengthened Loading
Lengthened = Open joint angles or eccentric bias
Example: assisted eccentric leg curls
5. Dynamic / Elastic Loading
Speed, reactivity, perturbation
Examples: Jumping, throwing, changing directions, running
6. Return to Task
Gradual exposure to sport or life-specific demands
Severity of injury and the injured tissue quality (muscle, tendon, ligament) will determine where you need to begin on this progression timeline.
Navigating Load: When to Push, When to Wait
Key Guidelines for Soft Tissue Rehab Progression:
The 3/10 Pain Rule: Keep pain during or after exercise below 3/10; if it exceeds this or lingers 24-48 hours, reduce load.
Pain Behavior: If pain is sharp, burning, or worsening, stop and rest. Consistent, manageable pain that dissipates quickly allows for continued progress.
Gradual Overload: Increase weekly volume or load by less than 10% to mitigate re-injury risk
The "80% Rule": End sessions feeling like you could have done slightly more to maintain consistency without over-overloading.
What to do if an exercise causes a 3+ out of 10 pain response
Reduce workload
Reduce range of motion, if applicable
Rest from activity
If recurrent, regress the exercise
Weeks 12+: Mitigate Re-Injury Risk
Whether or not you’re doing rehab work, most injuries feel better by the 12-16 week mark.
“Feeling better is not the same as full, structural healing. ”
It can take up to a year for tissue to regain — and if you’re doing your rehab, surpass — the structural integrity and strength the tissue had before injury.
Your Best Bet Injury Risk Mitigation Payout Pathways
Manage Menopause symptoms
Protect sleep quality & quantity
Take recovery days
Manage work-home-life stress
Eat and drink enough to repair and build metabolic tissue
“How could I let this happen 😥…”
Shame spiraling or blaming is not the best use of your energy immediately post-injury.
Objectively looking at what was different about ‘right now’ can help you start to hypothesize what led to your injury, and what changes you could implement when you get back to post-injury training.
Here are some common pathways:
1. Increased stimulus applied
No graded exposure after time off or a previous injury = you jumped right back in at the same workloads you did after a 2-week break off or being sick.
Excessive increases in volume (sets x reps x weight), tension, speed, or exercise complexity.
Large load jumps (e.g., +20 lb on your squat each week). We want a gradually progressive overload of 2-5% week-over-week.
A “I felt good so I went really hard” workout
2. Suppressed recovery
Poor sleep
High life stress
Inadequate time between demanding sessions
Under-fueled training energy (Carbs) and/or muscle repair (protein)
3. Reduced functional capacity
Loss of mobility or flexibility
Reduced strength in key ranges
Poor strength balance between tissues
4. Impaired movement variability
Longer desk hours recently
More or longer drives or flights
Training patterns that are too repetitive or redundant
5. Irritated physiological systems
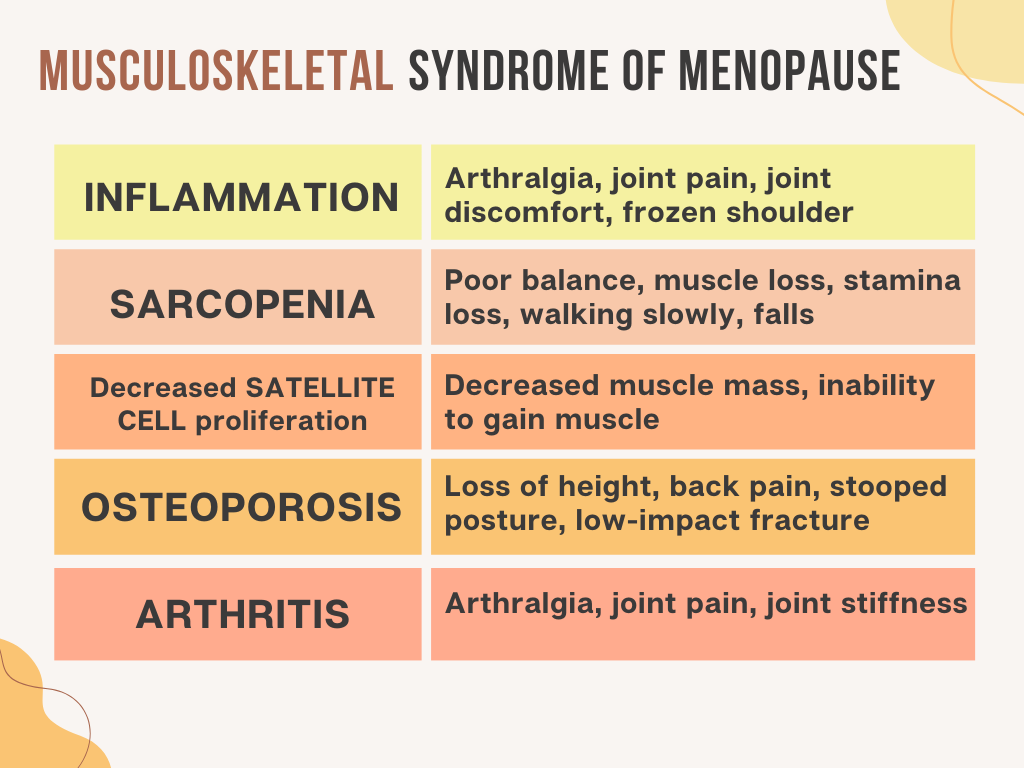
Musculoskeletal changes associated with menopause
Medication changes
Autoimmune flares
Nervous system dysregulation (over- or under-arousal)
Gut inflammation
Hormonal shifts in pre-/peri-menopause
6. Psychological or belief triggers
Fear or guarding from a past injury
Hypervigilance and catastrophizing
Movement myths (e.g., “deadlifts are dangerous”)
7. Program–person mismatch
Current training program doesn’t match your current skill, tolerance, or life stress
Progressions are too aggressive
Example: performing a “heavy triple” the fourth time you ever back squatted
Example: going from zero to 50 box jumps in a week
*This is general knowledge information, not medical advice!
References
Musculoskeletal Syndrome of Menopause PMID: 39077777
How Injuries Happen
PEACE & LOVE: British Journal of Medicine https://bjsm.bmj.com/content/54/2/72
Post-injury Protein Intake PMID: 26553492