Cheat Sheet: GainZ, Body Composition for Menopause & Aging
Question: “Can I build muscle and lose fat during menopause?”
Answer: Yes, you can.
The strategy is no different in any phase of menopause
than it is for someone in their 20s, or for that of a man.
But it requires a more deliberate approach than before menopause.
Here’s How
Step 0. Manage Menopause Symptoms
Menopause-related sleep disruptions and fatigue will lead to decreased physical activity, more food choice struggles, decreased training output, all which may lead to increased fat accumulation.
Symptom Management Tools:
Menopause Hormone Therapy (MHT = Estrogen + Progesterone, Testosterone)
Or Non-hormone treatments for Vasomotor Symptoms
Strict sleep hygiene
Alcohol reduction or elimination
Step 1. Trigger Building + Recovery
Consistently practice behaviors that trigger the body to “decide” to utilize food for building lean tissue.
Adequate & good quality Sleep
Train Strength & Power — 2-3 times per week PMID: 41687563
Enough Protein — 0.7 - 0.8 grams per pound of body weight, or 1-2 palm-sized servings per meal
Enough Carbs — 1 - 2.5 grams per pound of body weight, about ¼ of your plate for fruits, starchy carbs, & grains
2. Keep the Sink Un-Clogged
Practice behaviors that will promote building & recovery to continue.
N.E.A.T. -- Non-Exercise Activity Thermogenesis, AKA whole body movement. 6-8K steps per day.
Hydration — Drink to thirst, or if doing endurance activities/sports meet an oz. goal
Fiber - ~22 - 40g per day, or ½ of your plate with veggies
3. Play the Long Game
6 Months: you start to notice the hint of change in how clothes fit.
1-2 Years: others start to notice.
After two years: progress slows, but is still happening with progression, consistency, & patience.
3. Understand the Nuance
That research is still evolving our understanding of the role of gonadal hormones in performance training
That my main job isn’t research, and this info isn’t complete or flawless
That every body is different, and an 80 year old body won’t look or function exactly like its 45-year-old body
What to do if you don’t want to see actual change

These methods = Rearranging the deck chairs on the Titanic
Try to eat less. Menopause requires better fueling, not more restriction.
Try to wait out peri-menopause+ symptoms.
Believe in Spot Reduction. Example: doing ab exercises to lose belly fat.
Expect any benefits from Supplements like caffeine, Omega-3 s, adaptogens, vitamin infusions, probiotics, oral peptides, botanicals like Black cohosh, stimulants like L-Carnitine, Collagen…
Avoid spiking your cortisol or eating high glycemic index foods.
Tell yourself it’s too late to start making changes. It’s never too late!
Change nothing because you can’t do every single step “perfectly.”
BREAKDOWN: Why we gain weight in mid-life
It’s more complex than calories in/out.
Reason 1. “Effects of Aging”
Weight gain is primarily driven by muscle loss, reduced physical activity, and inadequate protein intake. Which becomes a vicious cycle. PMID: 35574515 PMID: 12145025, PMID: 26883880, PMID: 23867520
In the US, adults gain an average of 0.5 - 2 pounds per year through mid-life. Women typically gain weight at a higher rate and for a longer duration than men.
While men gain weight in a gradual & linear pattern, women tend to gain weight before and after the menopause transition (MT), with a redistribution of fat mass during MT. PMID: 1985614
TLDR: weight gain happens from moving less, eating insufficient protein, and losing muscle.
And women gain more weight than men.
Worth noting: this info is from population research data, and may not represent you. Approx. 50-80% of Americans don’t meet recommended nutrition and physical activity guidelines.
Reason #2: Effects of Menopause
Menopause doesn’t directly cause weight gain. 30843880, 22978257, 11910598, 10746891
It does increase signals for the body to lose muscle and gain fat, altering relative body composition. PMID: 30843880, 34898344, 11004935
Hormone Therapy alone doesn’t stop muscle loss, fat accumulation, or weight gain. PMID: 12055317
Muscle quality appears to shift (increased fat & connective tissue). PMID 41275401
Reduced neuromuscular function for force production PMID: 40349308
Hormone status doesn’t explain differences in metabolic rate https://doi.org/10.1016/j.numecd.2026.104637, PMID: 37265230
TLDR:Menopause is not directly responsible for weight gain during menopause, and has
a modest but statistically significant influence on body composition changes.
So…
“If Menopause plays almost no role in weight gain,
but women gain more weight than men in the long-term, what is to blame?”
Just my Hypothesis:
Women tend to gain more weight due to the contribution of menopause transition-caused body re-composition (muscle decrease & fat increase), in addition to the debilitating effect of Menopause Symptoms piled on top of the “normal effects of aging” and a dang busy life.
Also, the location of fat accumulation within the years preceding and following Menopause has a small but lasting snowball effect for long-term metabolic flexibility.
It’s arguable that factors such as reduced muscle quality, neuromuscular function, and reduced cross-sectional area don’t playing a role in longer-term body composition changes.
And you can still build muscle
= health, longevity, and metabolic currency
https://doi.org/10.1016/j.jsams.2026.03.002
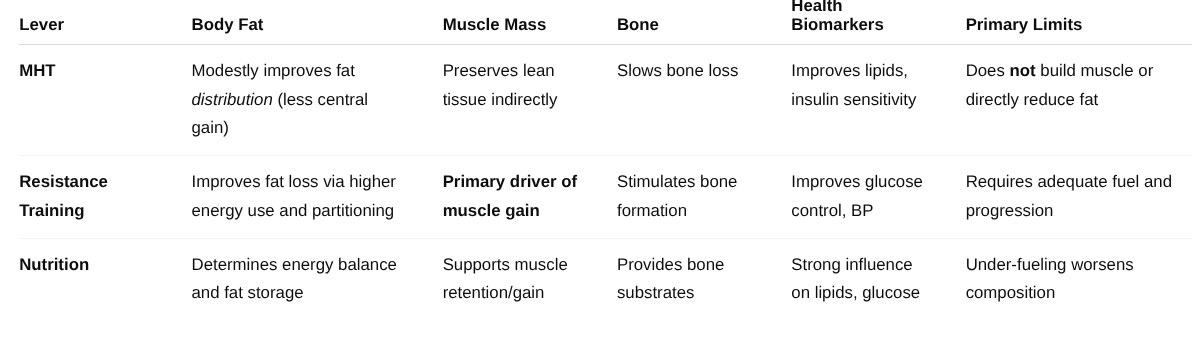
Breakdown of the influence & interplay of Hormone Therapy, Lifting Weights, and what you eat, on muscle and fat mass:
Hormone Therapy (MHT) is framed as protective, not transformative
Resistance Training is clearly the anabolic and structural driver
Nutrition is positioned as the enabler or limiter, not a stand-alone fix